In Canada, in 2021, more than 10,000 people died by by Assisted Suicide. Enabling sick people to end their own lives has increased ten-fold in that country in just 6 years, an alarming and revealing statistic.
Some people may take issue with my description of this shocking trend, preferring more euphemistic terms like ‘dignity in dying’ and avoiding realistic terms like ‘killing’, but it’s hard to avoid the cold hard facts of what actually happens.
(It’s also worth noting that the Irish Human Rights and Equality Commission, a left-leaning body, last year described ‘Dying with Dignity’ as a “potentially misleading” name for legislation that is really about allowing doctors to assist patients to end their own lives.)
In every case of physician assisted suicide, which is what is legal in Canada, a doctor – a person who has taken an oath to do no harm – administers a lethal injection into a patient in order to stop their heart.
As this recent article in the British Medical Journal spells out, a series of intravenous medications are given to firstly put the person to sleep, then numb them, then induce a coma – all before a fourth injection “stops breathing and heart function”.
“It usually takes 2-6 min to stop the patient’s heart,” the article explains – producing helpful flowcharts to guide practitioners in exactly how to end another human being’s life.
The annual report on Medical Assistance in Dying in Canada for 2021 shows that 10,064 people were euthanized in that year, a significant jump of 32% since the previous year.
It’s also a huge 10-fold increase in euthanasia deaths in just 6 years. Here’s how the information was presented by Health Canada – with an introduction by the Health Minister somewhat bizarrely saying he was “proud to present” the report.
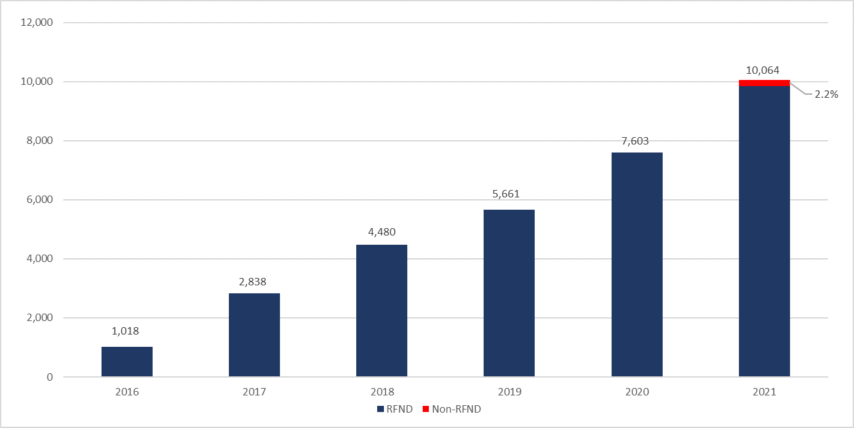
You’ll note that some of the patients whose lives were ended in 2021 were classified as “non-reasonably foreseeable deaths”. That’s because the law in Canada changed in 2021 to make it easier to access euthanasia – so that it was now available for “individuals for whom death was not reasonably foreseeable”.
The other criteria for euthanasia – having a serious and incurable illness, being an advanced state of irreversible decline in capacility, and experiencing enduring physical or psychological suffering – are examined according to outcomes in the 2021 report.
It’s revealing that the most commonly cited sources of suffering are not pain (which should be manageable with good palliative care) but the ‘loss of ability to engage in meaningful activities (86.3%), followed by loss of ability to perform activities of daily living (83.4%).’
What does it say about a rich and prosperous country like Canada that the sick and the elderly can’t get the support or engagement they need to continue with their lives? And does the move towards normalising euthanasia have an underlying, unspoken understanding that assisting people to die can be cheaper than providing healthcare?
Consider the case of Roger Foley from Ontario, who suffered from an incurable neurological disease. In 2018, he made audio recordings of hospital staff offering him medically assisted death, although he had actually repeatedly asked for assistance to live at home.
He was told he would be charged 1500 dollars a day if he continued to take up a bed in the hospital. It was horrifying.
The Life Institute has pointed to a paper published in a leading Canadian medical journal which claimed that millions could be saved in reduced health care spending by ‘medical assistance in dying’.
It “could result in substantial savings”, the authors noted approvingly. The paper was entitled “Cost analysis of medical assistance in dying in Canada” and was published in the Canadian Medical Association Journal.
“If Canadians adopt medical assistance in dying in a manner and extent similar to those of the Netherlands and Belgium, we can expect a reduction in health care spending in the range of tens of millions of dollars per year,” it claimed.
The emergence of such attitudes should be ringing alarm bells in Health Canada and in the legislature, but they may be considering instead the report from the parliamentary budget office in Ottawa which suggested that expanding access to Assisted Suicide would lead to nearly 1,200 more such deaths next year – and that this would be a saving of $149 million on end-of-life care spend.
As Life Institute explained in their “All about the money?” video last year, the attitude can also be found on this side of the Atlantic, pointing to “a disturbing paper published in the journal Clinical Ethics from two Scottish academics argued that Assisted Suicide “would save money and potentially release organs for transplant.”
Marie-Claude Landry, the head of Canada’s Human Rights Commission. is now warning that euthanasia “cannot be a default for Canada’s failure to fulfill its human rights obligations.
Her comments come in the wake of the “grave concern” expressed last year by U.N. human rights experts, who wrote that Canada’s euthanasia law had a “discriminatory impact” on people with disabilities.
A report by Associated Press this month on the death by euthanasia of Alan Nichols, who did not have a life-threatening disease, seems to add to the growing evidence that this is the case.
Maria Cheng from AP reports:
Alan Nichols had a history of depression and other medical issues, but none were life-threatening. When the 61-year-old Canadian was hospitalized in June 2019 over fears he might be suicidal, he asked his brother to “bust him out” as soon as possible.
Within a month, Nichols submitted a request to be euthanized and he was killed, despite concerns raised by his family and a nurse practitioner. His application for euthanasia listed only one health condition as the reason for his request to die: hearing loss.
Nichols’ family reported the case to police and health authorities, arguing that he lacked the capacity to understand the process and was not suffering unbearably — among the requirements for euthanasia. They say he was not taking needed medication, wasn’t using the cochlear implant that helped him hear, and that hospital staffers improperly helped him request euthanasia.
“Alan was basically put to death,” his brother Gary Nichols said.
As the euthanasia is normalised – and increasingly seen as an option to expensive healthcare – should we expect to see more and more such cases?
The real question might be when we start to care?