Introduction
Irish Minister of Health, Stephen Donnelly, has a habit of saying things that sound quite stupid. I suspect that is because he’s quite a stupid man and the things he’s saying are stupid. I’m not certain though – sometimes it can be hard to tell. Plenty of politicians have adopted dim-wittedness as a useful mask for malevolence (pun intended). Regardless, Donnelly sounded quite stupid last month when, in response to a journalist finally quizzing him on what the actual evidence was for face masks, he announced that there was “oodles of data”. It’s such a stupid sounding phrase that it actually gets under your skin. As we cringed uncomfortably at the Minister’s inane phraseology, we waited to see what he would offer. It took time but eventually his office did indeed provide the promised oodles.
In what follows, I sift through it all but let me start by saying that this is clearly a data dump, designed to drown the opposition in so much information that it overwhelms them. The desired outcome is that anyone looking at this list of data concludes that the sheer volume of it is proof enough of what is within. Masks must work – look how much data they have. So, in one sense, Donnelly’s office has lived up to its Minister’s claim – they have undoubtedly produced “oodles”. It’s just that they’re counting on you not looking too closely at what actually makes up the “oodles”.
There are generally three types of data in the dump. The first is not data at all, e.g., all the NPHET minutes and official recommendations. There is no data within them. They are not studies. They are just records of meetings and copies of letters that invariably state that masks work without ever offering any data to support that belief. The second type of data says the exact opposite of what Donnelly wishes the public to believe. Many of the referenced studies, as we shall see, conclude that there is little to no evidence to support the efficacy of masks. Finally, the third type of data is that faithful friend of the gullible – the weak, biased study that says very little but is trumpeted loudly by mask enthusiasts everywhere.
Let’s take a closer look at it all.
The Oodles of Data
The first reference provided is to this document that seems to serve as a general introduction to how the Department of Health makes its decisions. There’s no mention of masks anywhere in it so we can safely ignore.
- Minutes/Recommendations of the National Public Health Emergency Team (NPHET) Meetings
We won’t spend too long on these documents because, as mentioned, they’re not data – just records of meetings and the subsequent recommendations from NPHET to the Department of Health. The actual evidence they allude to in the minutes is considered in more detail in subsequent sections. However, a quick tour of the minutes is still illuminating.
Donnelly’s Office has listed 13 meetings where masks were discussed. The first from 14th May 2020 is complemented by a specific NPHET document on masking which contains two very striking quotations: the first from the European Centre for Disease Control (ECDC) which advises that:
“facial coverings could be considered but that evidence is lacking” (my emphasis)
and the second from the World Health Organisation (WHO):
“there is no current evidence to make recommendation for or against the use of cloth masks.” (my emphasis)
One is immediately struck by Donnelly’s office pointing us towards documents that openly acknowledge the lack of evidence for the very measure of which he is trying to convince us. The document on masking even goes on to talk of the danger of people being “misled into overestimating the importance of using a barrier mask or other face covering”. Given the hysterics that often met unmasked faces over the subsequent two years, I think we can safely say they failed to avoid this danger.
The minutes go further, referencing guidance from the Health Protection Surveillance Centre (HPSC) which acknowledges the potential harms of mandatory masking, highlighting the unsuitability of them for children, for “people with certain skin ailments” and for “people with dementia”. This leads to an important conclusion:
“It is essential that not wearing a mask does not lead to stigmatisation.”
It’s hard not to laugh, reflecting upon how these reasonable goals were shredded into confetti during the period of hysterical mask fetishism that followed. In the case of one maskless old age pensioner, subsequent NPHET policies saw her imprisoned and her very sanity publicly questioned in the national press.
But, just so we’re clear, NPHET conclude at this point in time that:
“the wearing of masks is not compulsory and should not be a requirement for an individual to access a premises or service.” (my emphasis)
They kept to that resolution for a good two months which brings us to the minutes of 14th July 2020 where NPHET are suddenly recommending the mandatory wearing of masks in retail environments (they were already mandatory on public transport at that point). They refer to the recommendations from the WHO and ECDC and “international studies” but fail to link to them or present any data whatsoever to explain this extraordinary change in approach. The last time any of their minutes discussed the evidence base for masks was 11th June 2020 (not referenced by Donnelly’s office) where they acknowledge that:
“the updated guidance from WHO notes that the widespread use of masks by healthy people in the community setting is not yet supported by high quality or direct scientific evidence and there are potential benefits and harms to consider.” (my emphasis)
So, no evidence but they recommended forcing people to wear them under the threat of imprisonment anyway. I guess that’s how Science works…
The 1st Oct 2020 minutes merely note NPHET’s recommendation that face mask regulations be extended. Again, no evidence or data is offered. The next reference is to minutes from 17th November 2020 but there are none for that date so I assume they mean 19th November 2020. These minutes note a recommendation to further extend face masks (to crowded outdoor areas). Again, no data is offered. There is a complementary NPHET document on masking but it merely details the existing mask legislation in Ireland and then summarises similar legislation around the world. The minutes from 25th November 2020 refer to a Health Information and Quality Authority (HIQA) report on masking which is significant and is considered below (see section 8).
There are six sets of minutes listed for 2021 (8th April, 25th August, 18th October, 11th November, 25th November, 2nd December). Where they mention masks, they are mainly in the context of whether the minimum age for mandatory masking should be reduced from the current 13 years of age. After repeatedly concluding throughout the year that the age should not be lowered (“The ECDC does not recommend the use of face masks in primary schools, as students may have “a lower tolerance to wearing masks for extended periods of time, and may fail to use the masks properly”” – Memo on the minimum age for the application of mask wearing), NPHET suddenly decide on 25th November that the minimum age should be lowered to 9 years of age. The sum of the evidence they offer is as per the below:
- “Studies directly evaluating the isolated effectiveness of mask wearing in children are limited.”
- “A small number of studies found that mask mandates in schools have been associated with lower incidence of SARS-CoV-2 infection, however, as other NPIs were often in place, it is difficult to determine the independent impact of mask wearing.”
That’s it. That’s why we masked primary school children. Based on nothing at all other than the desire of government apparatchiks to seen to be doing “something” rather than nothing.
The two referenced Minutes of 2022 (20th January, 17th February) simply chart NPHET’s sudden climbdown on mandatory masking. Suffice it to say, no evidence or data is provided one way or the other and very quickly afterwards, NPHET exited stage left – many of them into highly-paid senior positions in organisations towards whom they had channelled work during their time as publicly funded bureaucrats.
What these minutes demonstrate is that NPHET never had any convincing data or evidence for masking – something they openly admit several times in their meetings. For all their faults, NPHET repeatedly acknowledge the lack of evidence and limited data on masking. Their recommendation of them being made mandatory seems, from the minutes, to be a response to a worsening epidemiological situation rather than a genuine belief in their value. Facing that darkening outlook, they took refuge in aping the actions of other countries (whose measures they tracked heavily) in the belief that offering a worthless measure was better than offering none at all.
I wonder did Stephen Donnelly actually read this stuff?
[Donnelly’s office also provided a link to all the official NPHET recommendation letters to the Department of Health but as they are recommendations rather than data or even discussions of data, and insofar as they are merely distillations of the meetings already discussed above, I will not consider them here.]
This document is well over two years old now so obviously quite out of date. However, it is useful to consider it as the WHO would have been one of the chief organisations to whose authority NPHET appealed in justifying the introduction of forced masking in Ireland. In the section focusing on the available evidence for the effectiveness of community masking they cite two studies that apparently “provide evidence that the use of a medical mask can prevent the spread of infectious droplets from a symptomatic infected person (source control) to someone else and potential contamination of the environment by these droplets.”
- The first study concludes with the sentence: “we did not identify any trend in the results suggesting effectiveness of facemasks.”
- The second study is better insofar as it suggests “a potential benefit of medical masks” on respiratory illnesses and Influenza-like illnesses but the authors acknowledge that the trial is statistically irrelevant as it had less than 250 participants. It concludes with the line:
“The study indicates a potential benefit of medical masks for source control, but is limited by small sample size and low secondary attack rates.”
Well, that’s convincing!
Moving on, the WHO document states that “there is limited evidence that wearing a medical mask by healthy individuals in households, in particular those who share a house with a sick person, or among attendees of mass gatherings may be beneficial as a measure preventing transmission.”
As you’ll see, the word ‘limited’ does a lot of work here.
- The main study they rely upon is this meta-analysis of multiple random controlled trials which is quite useful as it is essentially a review of many of the other individual studies referred to elsewhere in Donnelly’s data dump. Its conclusion is unequivocal.
“Compared to no masks there was no reduction of influenza-like illness (ILI) cases (Risk Ratio 0.93, 95%CI 0.83 to 1.05) or influenza (Risk Ratio 0.84, 95%CI 0.61-1.17) for masks in the general population, nor in healthcare workers (Risk Ratio 0.37, 95%CI 0.05 to 2.50)” (my emphasis)
Are we sensing a pattern here? They state there is evidence (which there is) but when you actually look at the evidence it is either so paltry that it is utterly irrelevant or it is evidence in the exact opposite direction of what they are suggesting.
This isn’t exactly lying but it’s pretty close.
- The next study they mention is a meta-analysis of observational studies. Now when you see observational studies, you need to be careful. An observational study is just what it sounds like – you look at something and you make a conclusion based on what you see. It’s not really a study – it’s an observation and little more than that and it’s considered very, very weak science. Prof. Carl Heneghan, the Director of the Centre for Evidence Based Medicine at Oxford University dismisses this kind of evidence for masks as “weak observational evidence which has been shown over decades to have flaws”. To give one example of a famous observational study: The CDC famously trumpeted the Kansas Mask observational study which noted how, in summer 2020 after masks were introduced in Kansas, Covid cases stayed low. This, apparently, was strong evidence that masks worked. However, what happened after the (short) observational period of the study ended? Despite masks staying in place, cases went higher than they had ever been. This is why observational studies are generally junk. They’re a snapshot of a moment where any number of things might be affecting the situation you are observing.

- And having said all that, what did this meta-analysis actually say? They concluded, with low-certainty, that “face mask use could result in a large reduction in risk of infection.” So, in an analysis of weak, flawed studies they came out with a low-certainty could. Are you convinced? Because even the authors aren’t. They recognise their study’s own inadequacy, declaring that proper trials are needed to actually back this could up and recommend that their findings be used merely as interim guidance until such time as proper trails can be completed. How long exactly is interim? Two and a half years later and Stephen Donnelly is still appealing to such studies to make you wear a mask on the bus.
The WHO document also references six further studies, most of which are covered by the previously mentioned meta-analyses. But, for completeness’ sake, let me briefly list them here with their main conclusion.
- This study looks at hand-washing and facemasks together so it’s impossible to know what effects can be attributed to just facemasks. Even at that, the modest reduction in influenza transmission is admitted to be “not significant”.
- This study is not an RCT but rather another meta-analysis which focused on mass-gatherings and concluded that the effectiveness of masks “against specific infection remains unproven.”
- This study says masks, frequent hand-washing, and disinfecting living quarters, are “significantly protective factors” which sounds impressive but then you read the study and see that it is a Chinese telephone survey. In other words, this isn’t a study – it’s a load of cold calls taped together to look like a study.
- Overall, this study argues in favour of the effectiveness of masks but in its intention-to-treat analysis it admits that “there was no statistically significant effect of the M (masks) and MH (mask and handwashing) interventions.”
- Sigh, this study is another Chinese telephone survey where the people they phone say masks are great.
- This study isn’t a study at all but an attempt at seeing if a decent mask trial could be conducted at the annual Hajj pilgrimage to Mecca. They did a miniature version of it with less than 200 participants and concluded that – yes, you’ve guessed it – “laboratory results did not show any difference between the two groups (masked and unmasked).”
On to the European Centre for Disease Control (ECDC) and their recommendations for how to prevent transmission in health care settings. This particular document, which doesn’t consider community masking, simply states repeatedly that masks should be worn in every conceivable healthcare centre without even pretending to offer any data to back up that recommendation. It is, therefore, useless in this context.
Another document from the ECDC, this one on general transmission of Covid so it’s more relevant. That said, again you have to wonder if Stephen Donnelly’s office have actually read this stuff that they’re sending. The very first proper discussion of the evidence for masking states:
“There is no evidence on the usefulness of face masks worn by persons who are not ill to prevent infection from COVID 19, therefore this is not advisable. It is possible that the use of face masks by untrained people may even increase the risk of infection due to a false sense of security, inappropriate use of the mask, and increased contact between hands, mouth and eyes without hand washing.”
For some reason, this is what the Irish Minister of Health is offering as evidence for why he might mandate the general public to wear masks again.
Elsewhere, the document, like the previous one, talks of the usefulness of masks in healthcare settings without offering any data to support that belief.
This is the first document from the ECDC that is properly relevant and it is a broad examination of the evidence for masks both pre and post Covid. It’s actually quite good because, despite it naturally recommending masks, it recognises and acknowledges the paucity of the evidence in their favour – something our government has never done (at least not after summer 2020). To save ourselves meandering through all the studies referenced (most of which are considered elsewhere in this article), let us simply quote the start of the document which summarises all that follows.
The evidence regarding the effectiveness of medical face masks for the prevention of COVID-19 in the community is compatible with a small to moderate protective effect, but there are still significant uncertainties about the size of this effect. Evidence for the effectiveness of non-medical face masks, face shields/visors and respirators in the community is scarce and of very low certainty. (my emphasis)
Again, ask yourself how any reasonable person could offer these documents as justification for forcing the whole population to mask themselves, as Stephen Donnelly has done.
This document is a long list of recommendations by the ECDC in the context of increased vaccination and declining Covid circulation. It is not a discussion of evidence and so offers none for or against masking. Again, are they reading this stuff?
This is the document referred to in the minutes from NPHET’s meetings of 25th November 2020 (see section 2 above). It is a comprehensive examination of studies on masking by the Health Information and Quality Authority (HIQA) of Ireland. In discussing the evidence for masking, the document is littered with phrases like “uncertain” “low certainty evidence”, and “quality of the evidence from the studies was low.”
The document is long but it contains a useful appendix which summarises each of the studies considered. (Summary quotations below as per HIQA with my emphasis. My own comments in italics)
- Study 1 (RCT)- “not statistically significant” “Study not powered to detect small differences between the intervention groups. Largely based on self-report.”
- Study 2 (RCT)- “no statistically significant reduction” “Study not powered to detect small differences between the intervention groups. Largely based on self-report.”
- Study 3 (Observational) – “community-wide mask wearing may contribute to the control of COVID-19″ This was an observational study that observed that there were more Covid outbreaks in places that tended to have less masking (restaurants, bars, gyms) than in workplaces that used masks. From that, they theorised that masks may work. It’s a ridiculous study that places all the credit for differences in transmission on masks rather than the myriad other differences between the types of location compared. This is why, as per above, observational studies are, in the words of Prof. Heneghan, “weak” and “flawed”.
- Study 4 (RCT) – We considered this study already in Section 3 above. To repeat myself, the conclusion was: “This study looks at hand-washing and facemasks together so it’s impossible to know what effects can be attributed to just facemasks. Even at that, the modest reduction in influenza transmission is admitted to be “not significant”.
- Study 5 (RCT) – “No difference between groups” “Not powered to assess the relative efficacy of the interventions.” This was merely a feasibility study for Study 4.
- Study 6 (Observational) – This study suggests benefit of constant masking but as per HIQA “Study design precludes confirmation of causal relationship between variables…Findings are subject to memory recall, observer and information bias.” It’s largely meaningless in other words.
- Study 7 (Cross-sectional Study) – This appears to be a study on the impact of adolescent obesity on the 2009 Swine Flu. Its relevance is highly questionable. Like the previous study, it suggests a benefit to masking but again HIQA note that “Study design precludes confirmation of causal relationship between variables. Data collected by self-reported questionnaire. Ascertainment bias possible – previous infection or asymptomatic infection may have been missed.”
- Study 8 (RCT) – “There were minimal differences in incidence rates of URI, ILI or influenza among intervention groups” HIQA also include a long list of limitations of the study, too many to include here.
- Study 9 (Observational) – Chinese Phone survey already referenced in Section 3 above.
- Study 10 (RCT) – “Intent-to-treat analysis showed no significant difference in the relative risk of ILI in the mask use groups compared with the control group.”
- Study 11 (RCT) – This is a study on the potential usefulness of sucking tablets containing Lactoferrin and Lactoperoxidase for alleviating cold symptoms. As a side note, one subgroup was assigned masks and another wasn’t and the study noted “in subgroups with and without the face mask-wearing habit or handwashing habit, there were no statistical differences between the incidences of common cold symptoms of treatment and non-treatment groups.”
- Study 12 (RCT) – “Influenza transmission was not reduced by interventions to promote hand washing and face mask use.”
- Study 13 (Article) – This isn’t really a study about mask efficacy. As per its title (“Facemasks and intensified hand hygiene in a German household trial during the 2009/2010 influenza A(H1N1″) pandemic: adherence and tolerability in children and adults”) it just an exploration as to how the wearing of facemasks was tolerated and adhered to during an actual study.
- Study 14 (RCT) – Already reviewed above (See Section 3). My comment there: Overall, this study argues in favour of the effectiveness of masks but in its intention-to-treat analysis it admits that “there was no statistically significant effect of the M (masks) and MH (mask and handwashing) interventions.”
- Study 15 (Cross-Sectional Study) – This isn’t a study – it’s a questionnaire. And it claims very little anyway.
- Study 16 (Observational Study) – Another questionnaire, this one among schoolchildren in Japan. It says masks are great, suggesting a 9.9% efficacy of masks based on forms filled out by children…<insert eye roll smiley here>
- Study 17 (Observational Study) – Chinese phone survey already considered and dismissed in Section 3.
- Study 18 (Observational Study) – Not only is this another Chinese questionnaire that says masks are great, it’s a “retrospective” one which means the participants are not only at risk of bias (“Of course I wore my mask all the time, I am a good member of the Communist Party of China”) but they’re also at risk of not remembering whether they actually did or not.
- Study 19 (Observational Study) – Yet another Chinese questionnaire purporting to show masks are great. This one was online so at least they’ve stopped cold calling people to ask them if they wore their mask on the twenty-somethingth of last month. Try to think about the life of a typical Chinese citizen and how likely they are to be brutally honest when official people ask them about their compliance with whatever regulation they are supposed to be following.
- Study 20 (Observational) – This is a study based on a flight where 9 people who didn’t wear masks got infected with influenza. They say this suggests masks are a protective factor although admit that “a more comprehensive intervention study to accurately estimate this effect” is needed. I mean, what could be more comprehensive than 9 people on a plane??
The HIQA document then summarises another 18 Reviews, that is, not studies but reviews of studies. Analysing all of them is beyond the scope of this essay and as they are not actually data but merely reviews of data I feel justified leaving them aside. However, a brief consideration of the first listed review is worthwhile insofar as it validates the obvious conclusion towards which we are being led: that while weak, observational studies can sometimes suggest a positive impact of masks, the proper trials generally show that impact to be non-existent. That is borne out when the review concludes:
“Community mask use was associated with a potential decreased risk for SARS-CoV-1 infection in observational studies…Randomized trials in community settings found possibly no difference between N95 versus surgical masks and probably no difference between surgical versus no mask in risk for influenza or influenza-like illness.” (my emphasis)
This is an update to the previous document considering only those studies conducted between 24th June and 20th November 2020.
- The first study is a rapid review by the Norwegian Institute of Public health. In terms of direct evidence, it reviews 14 observational studies with the reviewers noting “a high risk of bias in all of the studies.” The review ultimately concludes that medical masks have a small protective effect but that “there is no reliable evidence of the effectiveness of non-medical facemasks in community settings.” So, even the reviews of likely biased, observational studies struggle towards a small positive effect for medical masks but no effectiveness at all for the types of masks everyone was forced to wear.
- The second study is merely an update to one already considered in the previous HIQA document (see Section 8, Study 1) and adds nothing to the evidence base. As HIQA state: The authors “noted that their original systematic review conclusion had been that the evidence on mask use in community settings and risk of SARS-CoV-2 infection was insufficient, and had been based on one study with methodological limitations. The most recent update concluded that the strength of the evidence remains insufficient.” (my emphasis)
- The third study is the notorious DANMASK-19 random control trial which was famously the first proper trial on the effectiveness of masks on Covid-19 infection. Its result was unequivocal – masks made no difference.
Next, the HIQA update references three new observational studies but fails to list them, concluding simply that they did not change the conclusions of the original HIQA review and they repeat the caveat that “the quality of the evidence is low”. They then move on to a smattering of other studies.
- The CDC’s hairdresser example – a description of how two hairdressers in Missouri wore masks and none of their customers were infected with Covid-19. This story was trumpeted by the CDC in 2020 as stellar evidence for the effectiveness of masks despite it not being a study, or a review, or anything at all other than a cute anecdote.
- Another observational study from Singapore “was unable to assess the effectiveness of community face mask use.”
- The next study discussed is actually the ridiculous Kansas study referenced above in Section 3 as a prime example of the inherent flaws of observational studies. It demonstrates perfectly how such studies can indicate an effect at the time of the study that is subsequently disproven.
Finally, the document discusses several mechanistic studies. Mechanistic studies are dismissed by Prof. Heneghan as readily as observational studies and even HIQA agree, noting that” they do not provide real-world evidence of the effectiveness of masks, and the transferability of their results to real-world settings is therefore unknown.” They are usually researchers in a lab spraying masked mannequins with aerosols (this is literally what one of the studies is). They are utterly silly and it is good that HIQA acknowledge that fact.
HIQA’s conclusion at the end of all that is important as it is a direct contradiction of Stephen Donnelly’s claim that there is “oodles of data” to support masking. They openly acknowledge what Donnelly will not, that there is an:
“ongoing absence of robust data to inform face mask recommendations”
Yet, not only did Donnelly recommend them, he forced men, women, and children to wear them and he passed legislation that saw some of those people go to prison for not doing so.
This document simply combines and summarises the data from the previous two HIQA documents. It has no new data.
This is a short document outlining how HIQA are going to review masking measures in other countries. I’m not sure whether the actual review was completed but it does not seek to gather any data on the effectiveness of masks. It merely seeks to compile a database on what other countries are requiring of their citizens. It, therefore, contains no data on masking.
In this document, HIQA consider whether the age for mandatory mask wearing should be lowered to include younger children. After discussing the epidemiological situation at the time, they turn to the efficacy of masks, noting that there is little update. They state that “observational and mechanistic evidence continues to point towards a beneficial effect, though the quantification of this effect remains highly challenging.” So, they say that two of the weakest and flawed forms of evidence point to them working but admit they can’t quantify it (presumably because whenever anyone does a proper RCT trial, it shows they don’t work.)
They go on to reference a few reviews, surveys, and observational studies – all of which suggest a potential small positive impact of masks but carry the usual caveats:
- “the independent effect of mask use is difficult to identify”
- “The studies described are insufficient for the determination of causality and not specifically designed to assess the effect of mask use.”
[HIQA fail to link or properly reference these studies so I can’t analyse them properly. However, it’s clear from HIQA’s document and their highlighting of the above quoted weaknesses that they offer little in the way of useful data.]
Given this lack of real evidence, HIQA decline to recommend lowering the age for mandatory masking.
- WHO, CDC, ECDC Links
At the end of the Department of Health’s Oodles of Data they throw in general links to the WHO, ECDC, and CDC websites. In case we weren’t already drowning in weak, puffed-up data, they decided to throw in one last massive pile of it.
For what’s it’s worth, the link to the WHO is to a page with a list of FAQs that include such banal entries as:
- When should masks be worn by the public? (Always)
- What kind of mask should the public wear? (Anything really)
- How should I put on, wear and take off a medical mask? (Act as if it is nuclear waste)
- Should I wear a mask while exercising? (Interestingly, they admit the answer is no to this one, even when in an area of high transmission, due to the risk of “reducing your breathing capacity.” I thought that was a conspiracy theory.)
There’s no data in any of the answers to these questions. There’s not even any argument, just bland boiler plate recommendations. Even the one question that might provoke some actual data – “Why should people wear masks?” – simply results in a dogmatic pronouncement of their effectiveness to “save lives”.
One of the CDC links is similar although it contains a disturbing “Find a Mask Near You” tool that will direct you to the nearest mask based on your geographical location. I find myself wondering if I could use it to navigate my way through the day without having to see one of the useless things.
The other CDC link is more substantial though, listing some actual studies, so we’ll have to consider it.
The first study mentioned is the Bangladesh Study. I’m glad this has come up. This study was the first RCT of the Covid era that actually supported mask use, or, at least, that’s what the media said. It bizarrely concluded that masks had a tiny effect (20 cases across 350,000 participants) in reducing Covid-19 infection but only in people aged over 50 years – surely an indicator straightaway that the study was producing nonsense data. Scepticism of the study, however, didn’t dissuade the media from trumpeting its weak conclusion in favour of masks.

This is in stark contrast to the DANMASK-19 study which struggled for months to even find a journal to publish its negative result for masks despite it being an efficiently and competently run trial. “When will it be published?” asked reporter Alex Berenson when the study failed to appear. “As soon as a journal is brave enough to accept the paper,” answered one of its lead investigators.
The scepticism the media had for DANMASK should, of course, have been reserved for Bangladesh as became clear once the full data from the latter study was revealed. A reanalysis of the study data showed “a large, statistically significant imbalance in the size of the treatment and control arms evincing substantial post-randomization ascertainment bias by unblinded staff.”
What does that mean? Basically, it means that the investigators were interfering (consciously or unconsciously) in the trial groups so as to favour their bias toward a positive evaluation of masks. And, to think, after doing that, they still only managed to come up with a miniscule benefit to crow about. The reanalysis concludes by stating that its conclusion “complicates drawing any causal link between masks and the observed decrease in population-rate of symptomatic seropositivity.”
I’ll say.
Nearly every other study listed by the CDC here is some version of an observational study so I’m not going to go through them. If it isn’t clear by now that observational studies are extremely weak data that can make anything look like it works depending on when and how you look, then let’s consider an example:
You go to the city of Manchester in England and you observe that people in the city who wear red football jerseys display a significantly increased likelihood of supporting Manchester United whereas people who wear blue football jerseys display a significantly increased likelihood of supporting Manchester City. You conclude, therefore, that red jerseys make people support Manchester United while blue jerseys make people support Manchester City. Congratulations, you’ve conducted an observational study and drawn a nonsense conclusion.

Obviously, the jersey isn’t the reason people support one team or the other – it is merely a symptom of the support they already have which exists independently of (and predates) the jersey they are wearing. In the same way, if an observational study shows that people that wear masks get slightly less Covid than those that don’t, might it not be the case that the mask-wearing is merely a symptom of that person’s increased vigilance when it comes to avoiding contracting viruses, a vigilance that is independent of (and predates) their mask wearing? In other words, the mask isn’t preventing Covid – it’s just something people who are already inclined towards actions that make them less likely to catch Covid are likely to wear (actions such as hand-washing and/or avoiding people).
The only other type of study listed by the CDC here are models. These are even worse data than observational or, even, mechanistic studies. A model study is where researchers tell a computer model or algorithm how effective masks are and then tell the model to calculate how many lives/cases would be avoided if X number of people wore such hypothetically effective masks. They are literally deciding at the start how effective masks are. There is absolutely nothing this type of model can tell us about mask efficacy, only what impact they would have if they were as effective as the researchers believe they are at the outset. It’s junk science of the highest order but it produces impactful, yet utterly meaningless headlines like the below so naturally the media love them.

The final link is to an ECDC document that acts as a kind of update to the one we already considered in Section 6. It adds 9 new studies, all of which are either observational, mechanistic, or already considered in this essay so, thankfully, there’s nothing for us to consider.
Conclusion
If you’ve read this far, I applaud you. As I said at the start, this is a data dump designed to drown you in data so you never see the truth. However, this long slough through it has hopefully given you an idea of what that truth is. The Government’s conviction that masks are an effective intervention rests on an incontinent stream of irrelevant rhetoric and schizophrenic observational and mechanistic studies – all of which struggle their way towards suggesting a potential, miniscule benefit for masking that is completely contradicted by proper, high-quality random controlled trials.
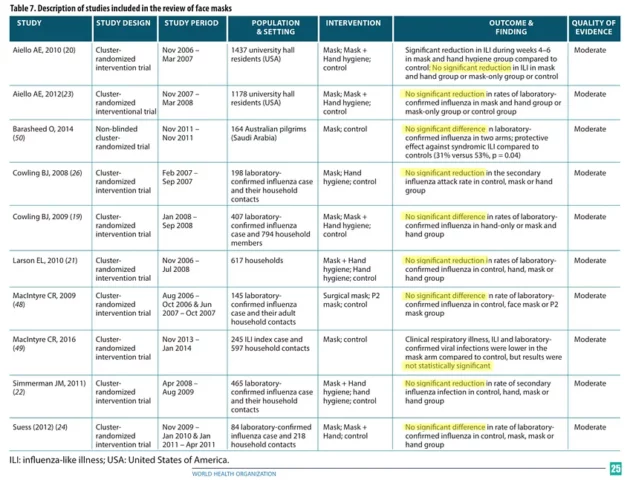
Observational and mechanistic studies do have a place in science. They can give an indication of a potential phenomenon that merits proper scientific investigation (usually via an RCT) but they are not in themselves capable of reaching any worthwhile conclusion about that phenomenon. That’s why so many of these studies end with the caveat that “additional high-quality studies are needed”. The thing is – we have already done many high-quality studies and they generally show that masks don’t work. A lot of people don’t want to accept that but time and time again, when we test masks properly, we keep seeing that they make no difference. Back in 2019, before the issue became so politicised and divisive, the WHO themselves carried out an analysis of available RCTs, concluding:
Ten RCTs were included in the meta-analysis, and there was no evidence that face masks are effective in reducing transmission of laboratory-confirmed influenza.
See below table for a breakdown of the conclusions of each study.
All of this, then, is the basis of evidence upon which Stephen Donnelly, not just recommended, but forced masks, at pain of imprisonment, upon the population. Can anyone honestly say that such an extraordinary interference in society was remotely justified by this data? And now, after two years of rabid masking, with Donnelly threatening to return to forced masking, do we have any compelling reason to overthrow the pre-Covid prevailing wisdom?
Let’s be clear, the forced masking of millions of people right across the world during a global pandemic should have provided the kind of data mask enthusiasts like Donnelly needed to prove their measure. In other words, if masks worked we would know about it by now. The indisputable data would be on the front page of every newspaper. But it’s not. All we have is Donnelly’s ridiculous appeal to “oodles of data” and then this data dump from his office that spectacularly fails to back up his claims.
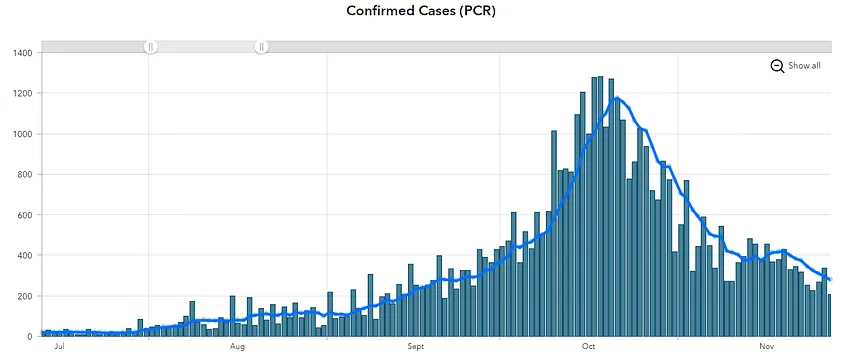
So, why, then, do we keep being told that masks save lives? Why did Ireland’s leader, Micheál Martin state on 27th November 2020 in an address to the nation that: “we introduced guidance on wearing masks indoors and this has had an incredibly positive impact”? The below graph starts exactly when masks were first introduced in Ireland (July 13th 2020) and ends on the date of Martin’s claim above. Every single metric we use to measure Covid (cases, deaths, hospitalisations, positive rate) was worse on November 27th than it was on the day masks were introduced, with a significant surge in between. He literally had nothing to base his claim on but he said it anyway. Why?
Ultimately, I would guess the reason Governments and Public Health Authorities still pretend masks work is the same reason we still pretend Santa is real. It makes a certain type of person feel better.
What type of person?
A child, of course.
Well, it’s time to grow up. We’re not children.
Santa isn’t real.
And masks don’t work.

Damian Bruce
The text was originally published here in Damian Bruce’s Substack “Ragged Lines”, and was produced after Gript’s Ben Scallan asked Irish Health Minister Stephen Donnelly what actual data he had to support a return to forced masking after he threatened reintroducing the measure.